Prostate cancer proves a common recurrence for many1-3
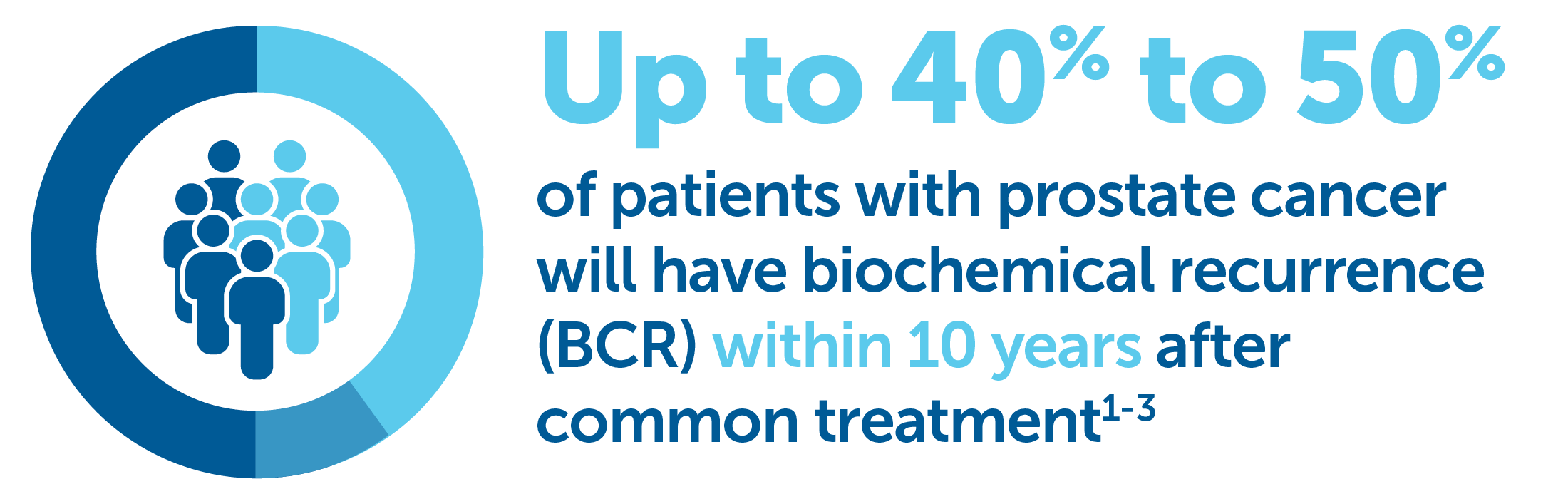
Of patients who experienced BCR1-3
-
20% to 40% had undergone a radical prostatectomy
-
30% to 50% had been treated with radiation
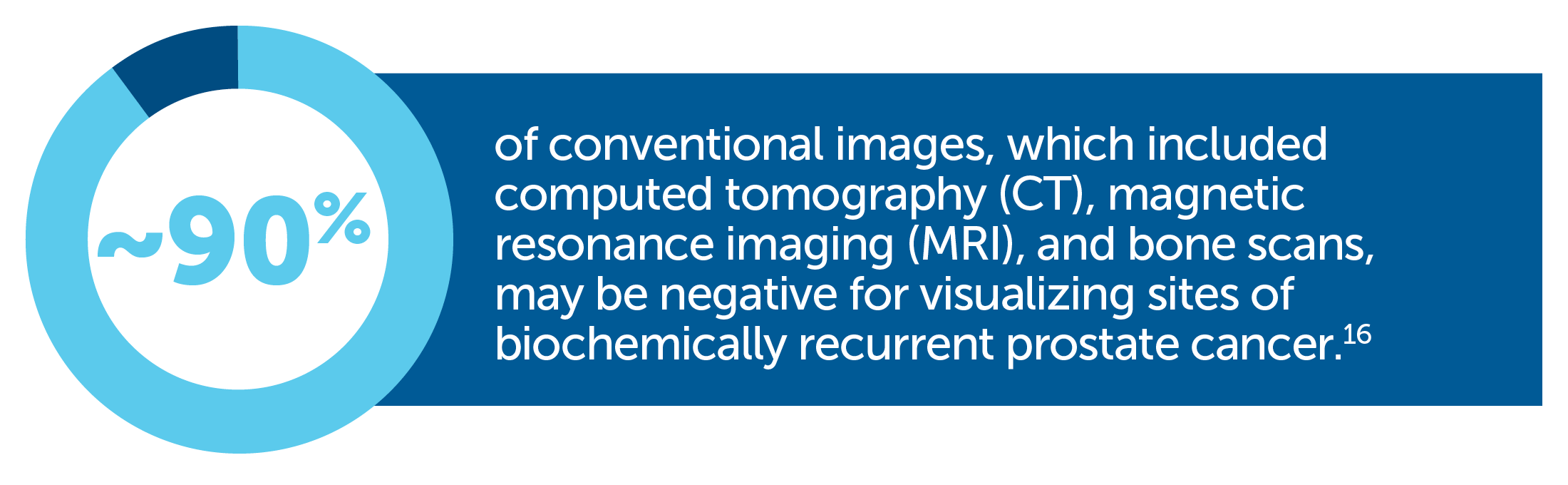
Accurate imaging techniques are critical for clinical decision-making
Many traditional approaches still present challenges
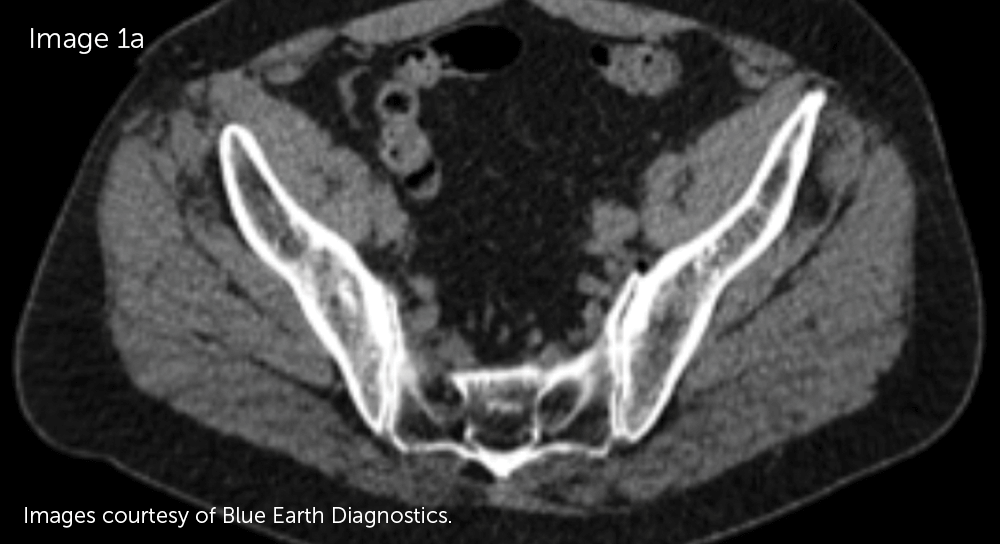
Limitations of the most common current imaging procedures6
|
May not detect small tumors |
Some imaging procedures may be unable to detect recurrent prostate tumors <1 cm in size or when PSA levels are <10 ng/mL—when cancer may be more effectively managed or treated with localized therapy7-12 |
|
Difficult to use |
Some imaging procedures can be time-consuming or present challenges for reproducibility of results13-15 |
|
May require multiple scans to evaluate all potential metastatic sites |
Bone scans, CT scans, and/or MRI may be necessary7 |

References:
- Paller CJ, Antonarakis ES. Management of biochemically recurrent prostate cancer after local therapy: evolving standards of care and new directions. Clin Adv Hematol Oncol. 2013;11(1):14-23.
- Darwish OM, Raj GV. Management of biochemical recurrence after primary localized therapy for prostate cancer. Front Oncol. 2012;2:48.
- Bruce JY, Lang JM, McNeel DG, et al. Current controversies in the management of biochemical failure in prostate cancer. Clin Adv Hematol Oncol. 2012;10:716-722.
- Chau A, Gardiner P, Colletti PM, Jadvar H. Diagnostic performance of 18F-fluciclovine in detection of prostate cancer bone metastases. Clin Nucl Med. 2018;43(7):e226-e231.
- Expert Panel on Urologic Imaging; Froemming AT, Verma S, Eberhardt SC, et al. ACR Appropriateness Criteria® Post-treatment Follow-up Prostate Cancer. J Am Coll Radiol. 2018;15(5S):S132-S149.
- Thompson IM, Valicenti RK, Albertsen P, et al. Adjuvant and salvage radiotherapy after prostatectomy: AUA/ASTRO Guideline. J Urol. 2013;190(2):441-449.
- Hricak H, Choyke PL, Eberhardt SC, Leibel SA, Scardino PT. Imaging prostate cancer: a multidisciplinary perspective. Radiology. 2007;243(1):28-53.
- Kirkham AP, Emberton M, Allen C. How good is MRI at detecting and characterising cancer within the prostate? Eur Urol. 2006;50(6):1163-1174.
- Schiavina R, Ceci F, Borghesi M, et al. The dilemma of localizing disease relapse after radical treatment for prostate cancer: which is the value of the actual imaging techniques? Curr Radiopharm. 2013;6(2):92-95.
- Wolf JS Jr, Cher M, Dall’era M, Presti JS Jr, Hricak H, Carroll PR. The use and accuracy of crosssectional imaging and fine needle aspiration cytology for detection of pelvic lymph node metastases before radical prostatectomy. J Urol. 1995;153(3 pt 2):993-999.
- Merdan S, Womble PR, Miller DC, et al. Toward better use of bone scans among men with early-stage prostate cancer. Urology. 2014;84(4):793-798.
- Ikonen S, Kärkkäinen P, Kivisaari L, et al. Magnetic resonance imaging of clinically localized prostatic cancer. J Urol. 1998;159(3):915-919.
- Hegde JV, Mulkern RV, Panych LP, et al. Multiparametric MRI of prostate cancer: an update on state-of-the-art techniques and their performance in detecting and localizing prostate cancer. J Magn Reson Imaging. 2013;37(5):1035-1054.
- Aparici CM, Carlson D, Nguyen N, Hawkins RA, Seo Y. Combined SPECT and multidetector CT for prostate cancer evaluations. Am J Nucl Med Mol Imaging. 2012;2(1):48-54.
- Taneja SS. Imaging in the diagnosis and management of prostate cancer. Rev Urol. 2004;6(3):101-113.
- Choueiri TK, Dreicer R, Paciorek A, et al. A model that predicts the probability of positive imaging in prostate cancer cases with biochemical failure after initial definitive local therapy. J Urol. 2008;179(3):906-910.
INDICATION
Axumin® (fluciclovine F 18) injection is indicated for positron emission tomography (PET) imaging in men with suspected prostate cancer recurrence based on elevated blood prostate specific antigen (PSA) levels following prior treatment.
IMPORTANT SAFETY INFORMATION
- Image interpretation errors can occur with Axumin PET imaging. A negative image does not rule out recurrent prostate cancer and a positive image does not confirm its presence. The performance of Axumin seems to be affected by PSA levels. Axumin uptake may occur with other cancers and benign prostatic hypertrophy in primary prostate cancer. Clinical correlation, which may include histopathological evaluation, is recommended.
- Hypersensitivity reactions, including anaphylaxis, may occur in patients who receive Axumin. Emergency resuscitation equipment and personnel should be immediately available.
- Axumin use contributes to a patient’s overall long-term cumulative radiation exposure, which is associated with an increased risk of cancer. Safe handling practices should be used to minimize radiation exposure to the patient and health care providers.
- Adverse reactions were reported in ≤1% of subjects during clinical studies with Axumin. The most common adverse reactions were injection site pain, injection site erythema and dysgeusia.
To report suspected adverse reactions to Axumin, call 1-855-AXUMIN1 (1-855-298-6461) or contact FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Please see Axumin full Prescribing Information.