The efficacy of Axumin® (fluciclovine F 18) injection was established in clinical studies1
The FDA-approved prescribing information provides summaries from 2 clinical studies of Axumin, including an evaluation of 105 images by 3 independent readers who were unaware of the clinical details of each patient and whether the biopsy of the prostate/prostate bed or suspicious lesions on imaging were positive or negative for cancer. The charts illustrate the correctly predicted biopsy findings.
Clinical studies were based on patients with elevated prostate specific antigen (PSA) levels following radical prostatectomy and/or radiotherapy. Patient PSA levels seemed to affect results with, in general, lower PSA levels correlating more frequently with negative scans than with positive scans.1
Pivotal Study
High levels of accuracy seen with Axumin
In a retrospective, observational study evaluating the efficacy and safety of Axumin PET imaging in patients with suspected biochemically recurrent prostate cancer.1
Accuracy across all regions1*
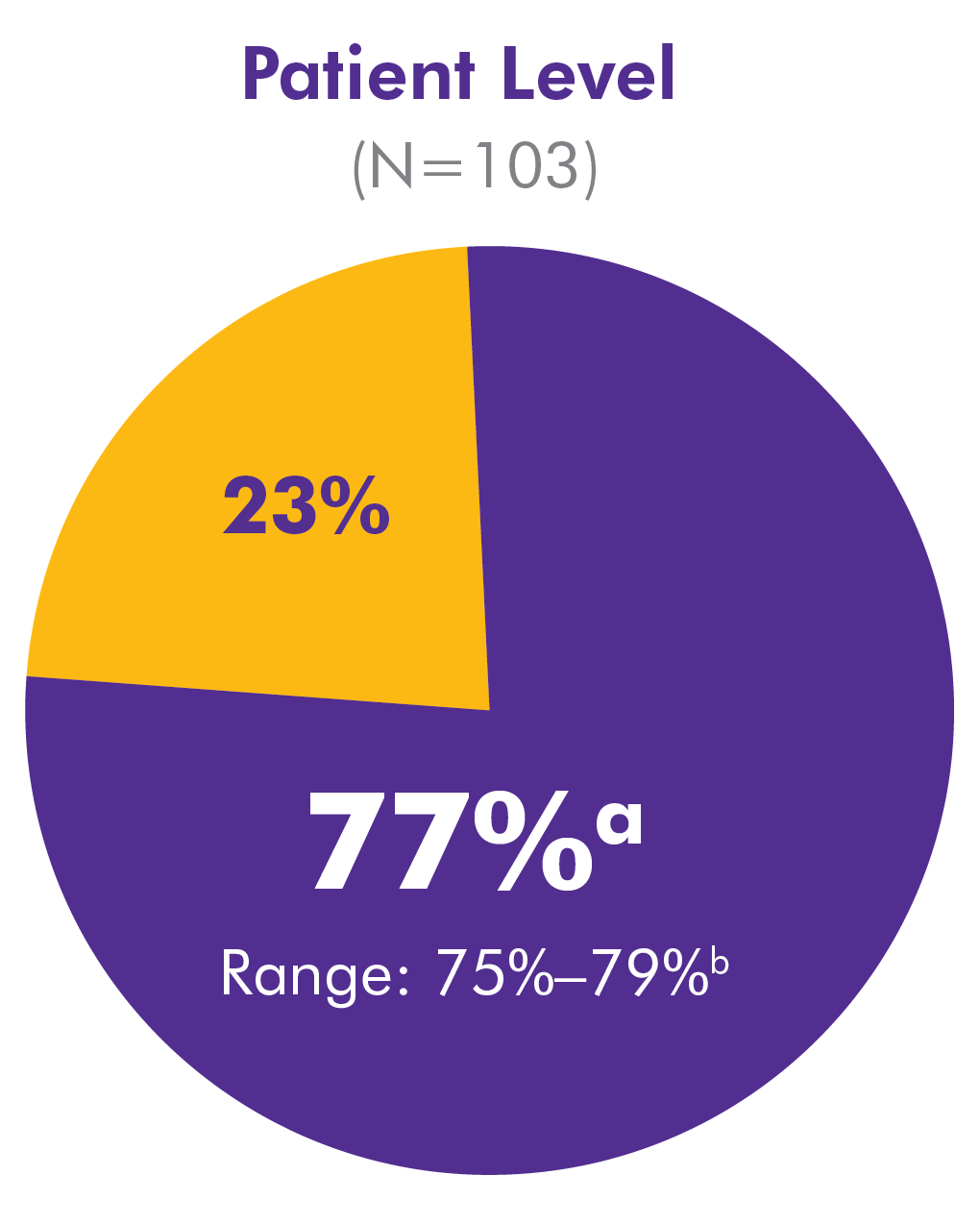
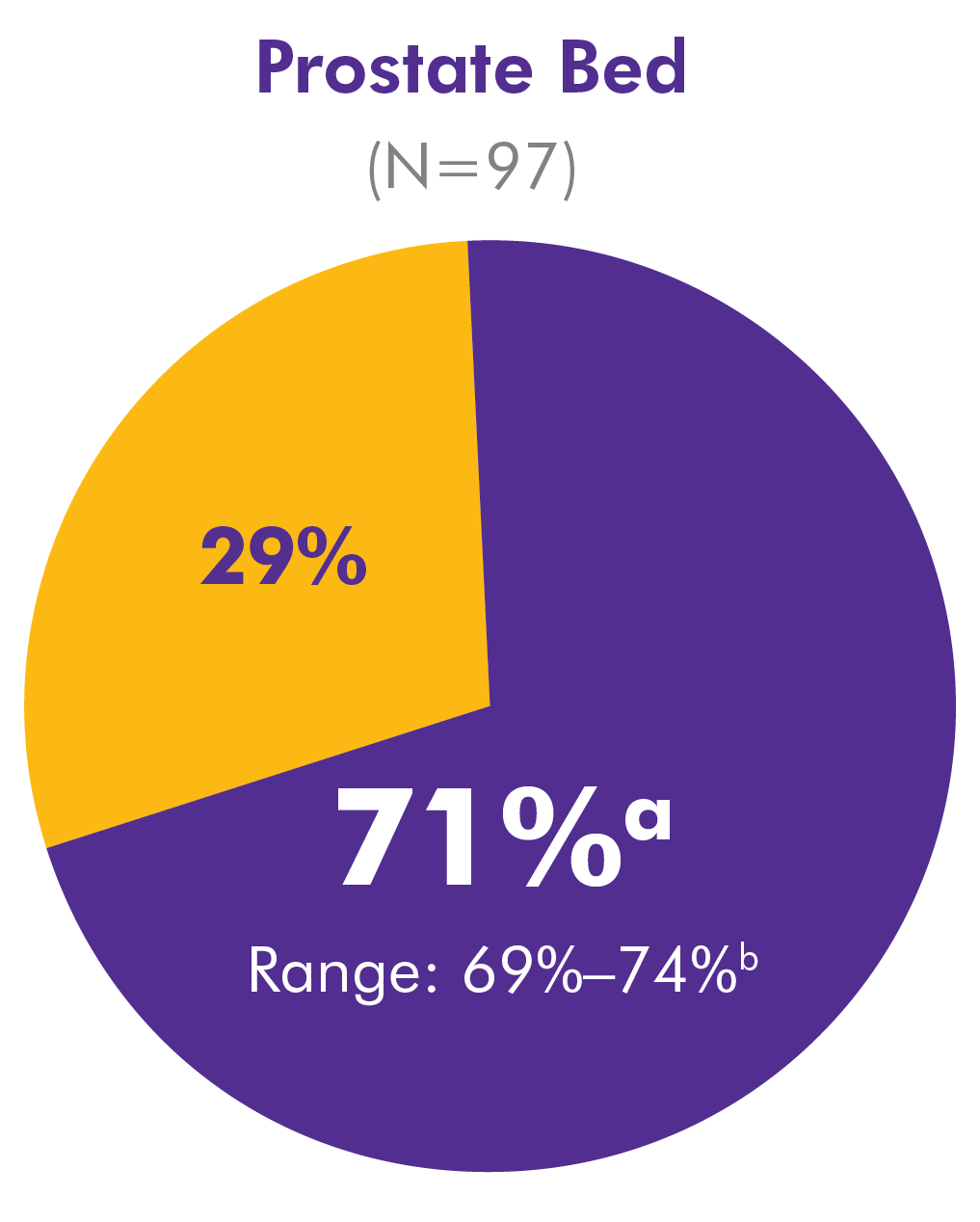
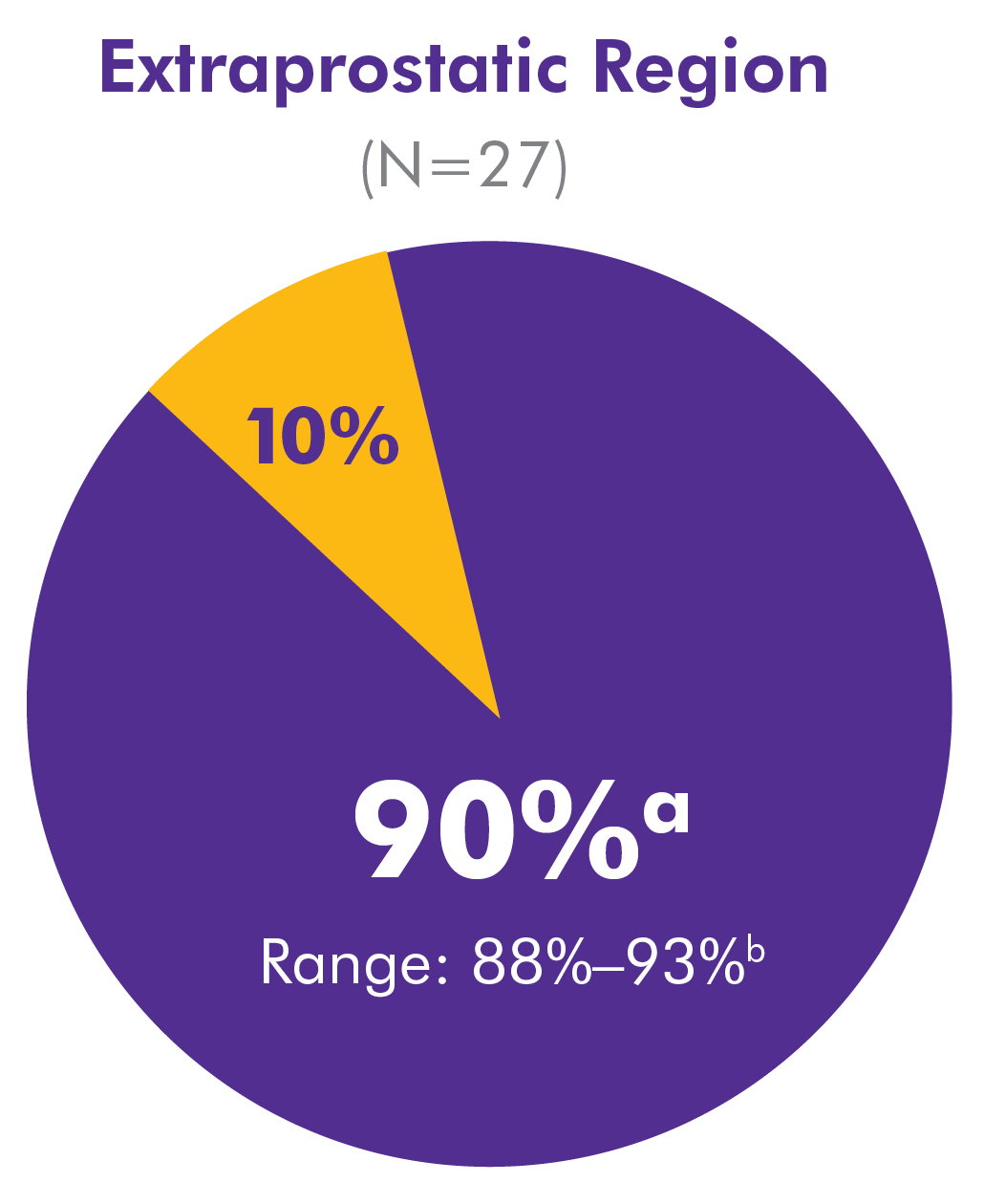
*105 images were evaluated by 3 independent readers who were unaware of the clinical details of each patient and whether the biopsy of the prostate bed or suspicious lesions on imaging were positive or negative for cancer. N is averaged across the 3 readers.
aAccuracy average of 3 blinded readers.
bAccuracy range across 3 blinded readers.
Accuracy = true positive + true negative/true positive + false positive + true negative + false negative.
Journal of Urology (Bach-Gansmo)
High detection rates even with low PSA levels
In a multicenter, retrospective, observational study of the efficacy and safety of Axumin PET/CT in 596 patients with biochemical recurrence2
Distribution of recurrent and metastatic sites in men with positive Axumin scans (N=403)2:
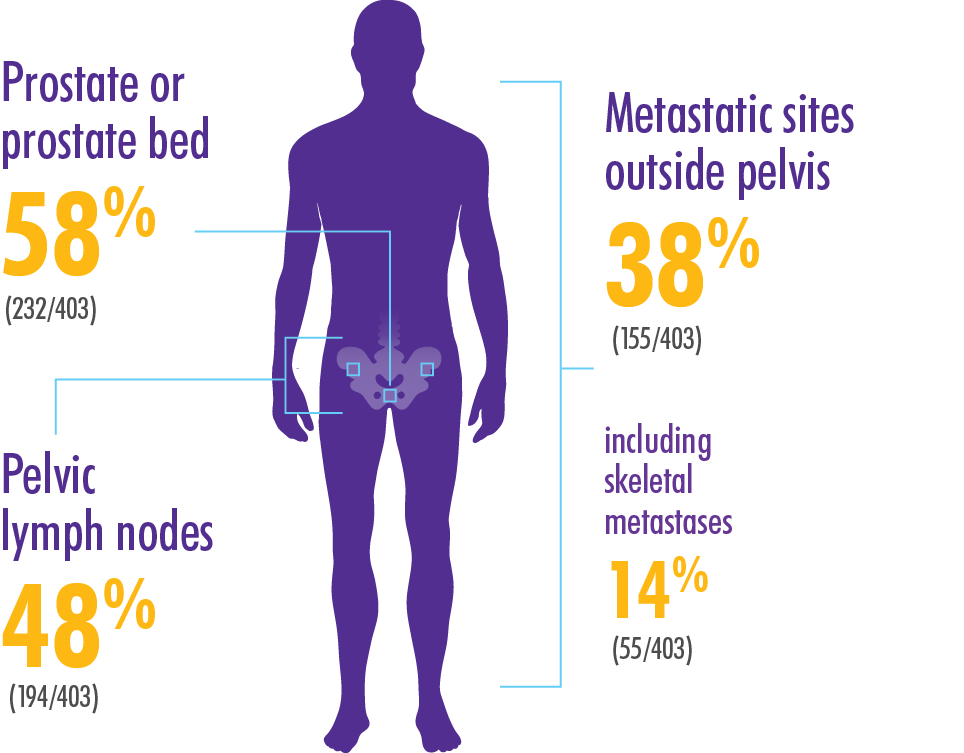
68% (403 of 595 scans) overall detection rate of recurrent prostate cancer2
High detection rate across PSA levels
Impact of PSA on Axumin PET/CT detection rate at subject levels in combined data set2
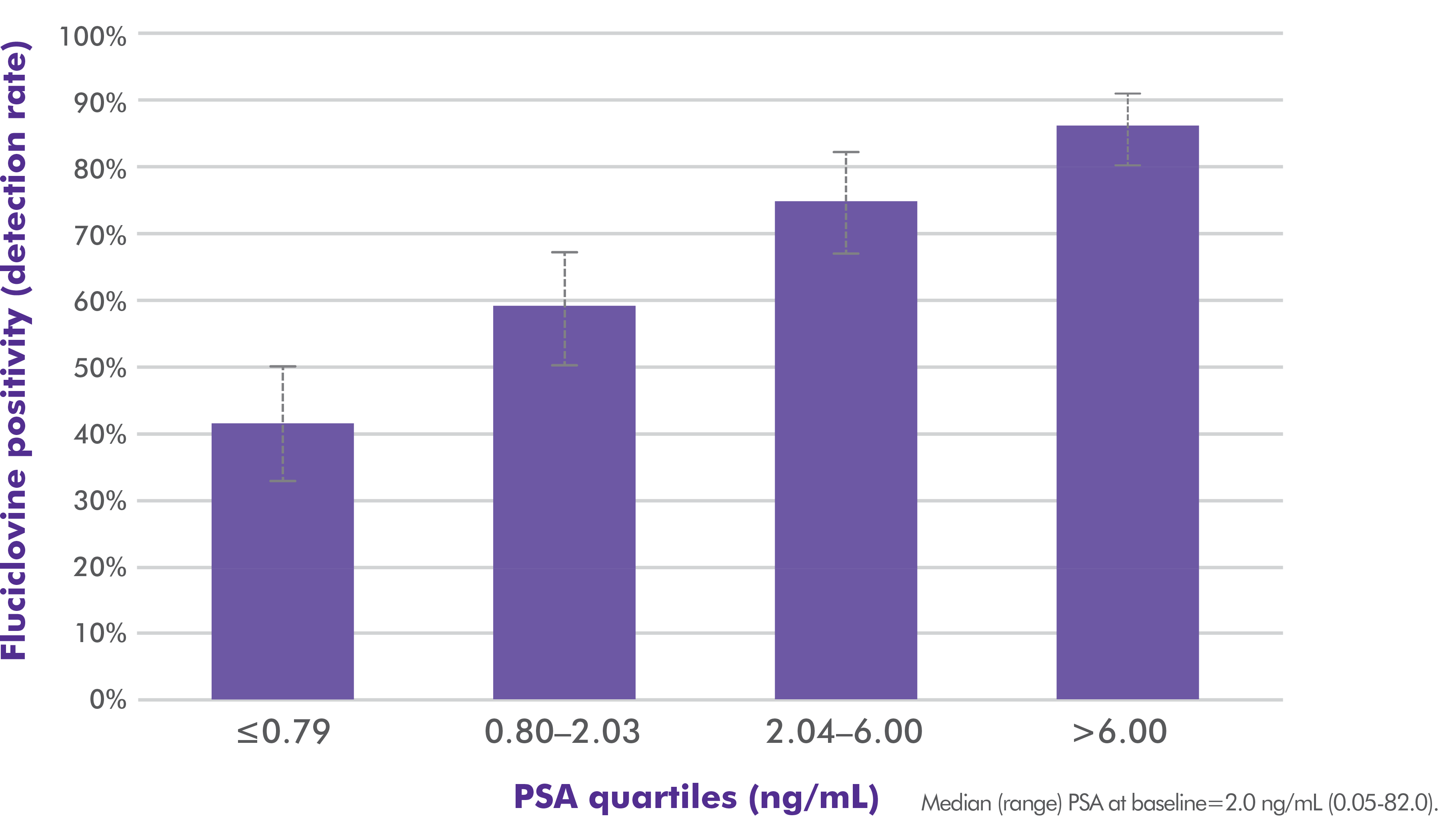
Detection rate of ~40% in patients with PSA levels ≤0.79 ng/mL, rising to ~60% at PSA 0.80‑2.03 ng/mL2
The positive predictive value (PPV) of Axumin in the prostate bed was 72% for prostate/bed involvement.2
American Journal of Roentgenology (Savir-Baruch)
High detection rate of recurrence correlated with increasing PSA levels
A retrospective cohort study of 152 men who had suspected biochemical recurrence of prostate cancer after receiving initial treatment and had an Axumin scan. Detection rates (DR) were calculated for whole-body, prostate and prostate bed, and extraprostatic locations. The influence of different factors (absolute PSA level, PSA kinetics, the Gleason score, and Gleason grade groups) on the DR were evaluated.3
Initial therapy received by patients (N=152)3
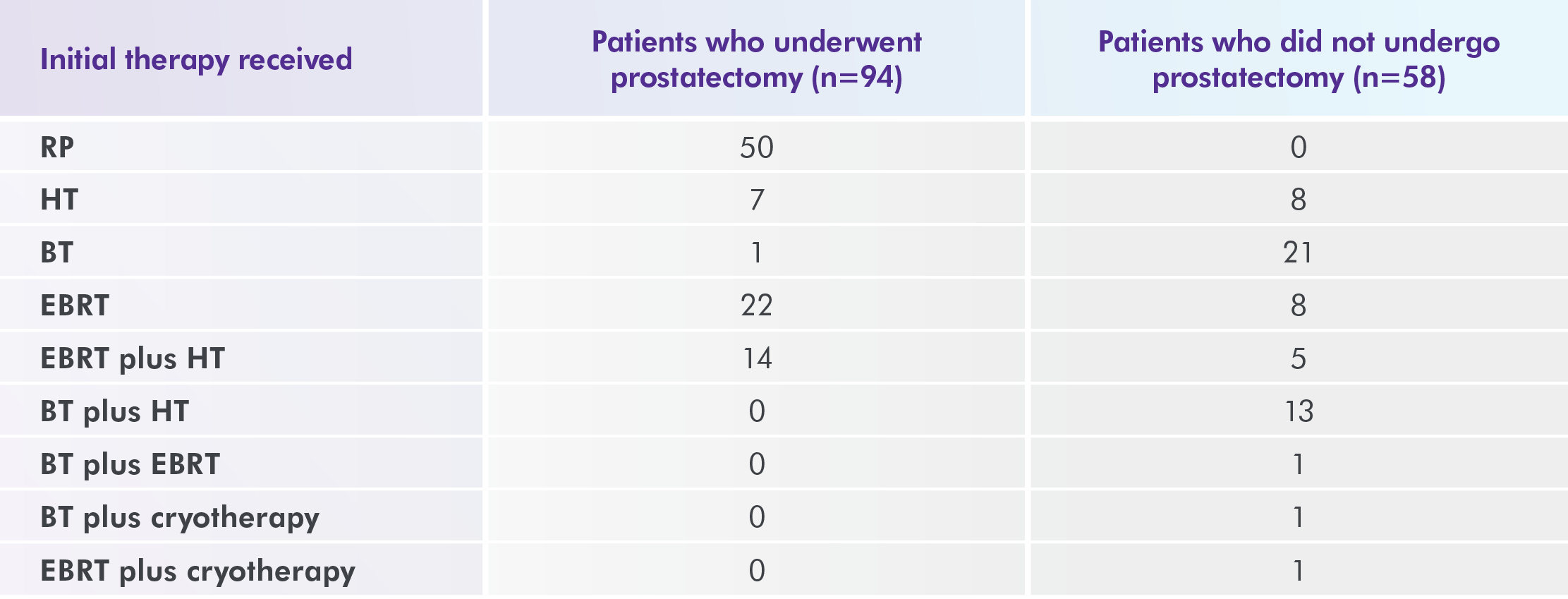
Note: Data are number of patients.
Abbreviations: BT, brachytherapy; EBRT, external beam radiation therapy; HT, hormone therapy; RP, radical prostatectomy.
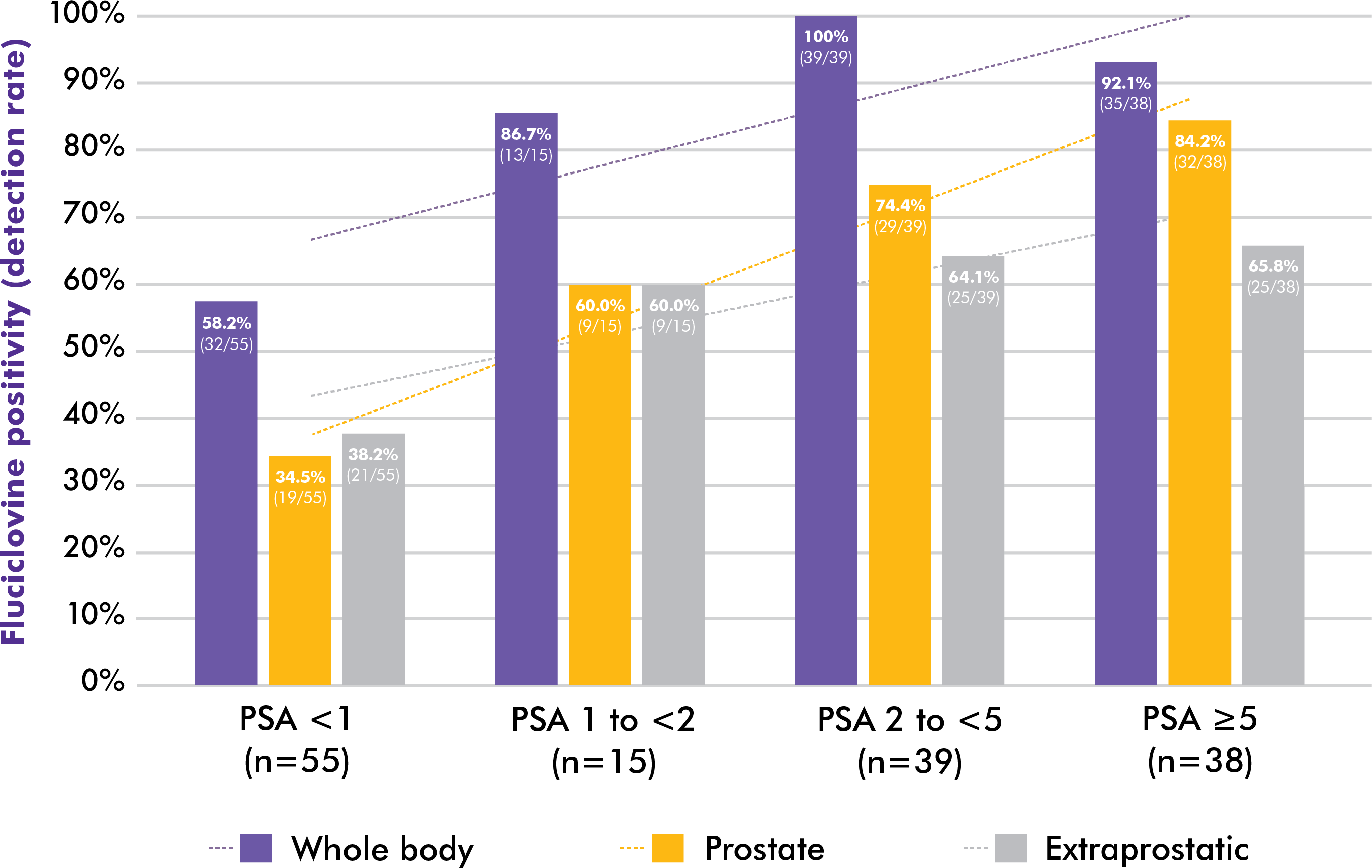
Axumin demonstrated an overall (whole-body) detection rate of 81%3
Of the 152 patients in the cohort:
- 61% (92) had positive findings within the prostate and prostate bed
- 55% (83) had positive findings in the extraprostatic region (lymph nodes, bone, viscera, or a combination of these locations)
Detection rates correlated with increasing PSA levels3
A linear increase followed rising PSA levels (P<0.001)3
PSA doubling time or velocity has no statistically significant effect on the detection rates of Axumin3
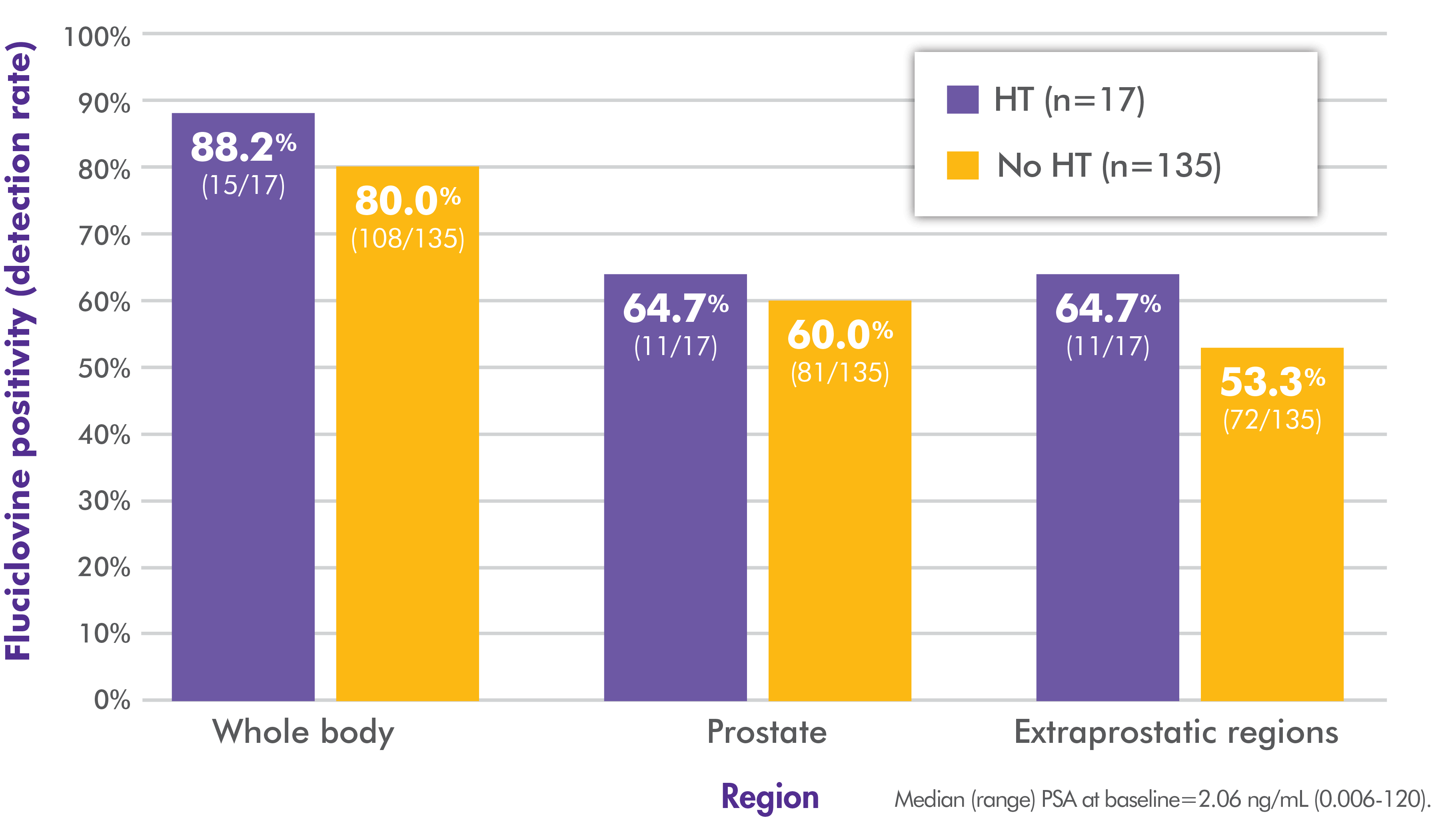
Similar detection rates seen regardless of hormone therapy status3
Detection rates with and without hormone therapy3
Likelihood of detecting extraprostatic lesions with positive Axumin findings significantly increased with an increasing Gleason score3
Safety data were not reported in this study
References:
- Axumin [package insert]. Oxford, UK: Blue Earth Diagnostics Ltd; July 2022.
- Bach-Gansmo T, Nanni C, Nieh PT, et al. Multisite Experience of the Safety, Detection Rate and Diagnostic Performance of Fluciclovine (18F) Positron Emission Tomography/Computerized Tomography Imaging in the Staging of Biochemically Recurrent Prostate Cancer. J Urol. 2017;197:676-683.
- Savir-Baruch B, Lovec P, Solanki AA, et al. Fluorine-18-labeled fluciclovine PET/CT in clinical practice: factors affecting the rate of detection of recurrent prostate cancer. AJR Am J Roentgenol. 2019;213(4):851-858.
INDICATION
Axumin® (fluciclovine F 18) injection is indicated for positron emission tomography (PET) imaging in men with suspected prostate cancer recurrence based on elevated blood prostate specific antigen (PSA) levels following prior treatment.
IMPORTANT SAFETY INFORMATION
- Image interpretation errors can occur with Axumin PET imaging. A negative image does not rule out recurrent prostate cancer and a positive image does not confirm its presence. The performance of Axumin seems to be affected by PSA levels. Axumin uptake may occur with other cancers and benign prostatic hypertrophy in primary prostate cancer. Clinical correlation, which may include histopathological evaluation, is recommended.
- Hypersensitivity reactions, including anaphylaxis, may occur in patients who receive Axumin. Emergency resuscitation equipment and personnel should be immediately available.
- Axumin use contributes to a patient’s overall long-term cumulative radiation exposure, which is associated with an increased risk of cancer. Safe handling practices should be used to minimize radiation exposure to the patient and health care providers.
- Adverse reactions were reported in ≤1% of subjects during clinical studies with Axumin. The most common adverse reactions were injection site pain, injection site erythema and dysgeusia.
To report suspected adverse reactions to Axumin, call 1-855-AXUMIN1 (1-855-298-6461) or contact FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Please see Axumin full Prescribing Information.