Axumin® (fluciclovine F 18) patient case studies
When presented with a negative or equivocal scan, Axumin provides clarity for decision-making in clinical management.1
Lymph Node Uptake
Clinical history:
- Age at diagnosis: 65
- Date of diagnosis: 10/2014
- PSA at diagnosis: 5.6 ng/mL
- Gleason score: 3+4=7
- Initial treatment: Radical prostatectomy (11/2014)
- Final pathology: pT3b, N0, M0; 4+3=7 with tertiary pattern 5; extraprostatic extension, positive margins and bilateral seminal vesicles
- Post treatment nadir PSA: <0.10 ng/mL (1/2015); undetectable
1st PSA recurrence and treatment:
- PSA: 0.48 ng/mL (4/2015)
- Salvage radiotherapy (11/2015)
- PSA: 0.50 ng/mL (2/2016)
2nd PSA recurrence:
- PSA: 2.2 ng/mL (8/2016)
Conventional imaging results:
- Negative Tc-99m bone scan (9/2016)
- Negative MRI of prostate and prostate bed (9/2016)
Planned clinical management:
- Salvage radiotherapy to the prostate bed
Details associated with decision to refer patient for an Axumin scan:
- Rising PSA post-prostatectomy and salvage radiotherapy
- PSA at time of Axumin scan: 7.0 ng/mL (9/2016)
Axumin imaging interpretation:
- Positive Axumin PET/CT: Fluciclovine F 18 uptake demonstrated in para-caval and right retrocrural lymph nodes (10/2016)
Final management plan:
- Bicalutamide and leuprolide
Clinical follow-up:
- PSA 0.1 ng/mL (2/2017)

Axumin imaging revealed para-caval lymph node malignant uptake
Lymph Node SUV(bw)max: 2.7
Blood pool SUV(bw)mean: 1.0
Axumin imaging revealed retrocrural lymph node malignant uptake
Lymph Node SUV(bw)max: 3.6
Blood pool SUV(bw)mean: 1.0
Provided by:
David Josephson, MD, FACS Tower Urology Institute for Minimally Invasive and Robotic Surgery / Attending Surgeon / Cedars Sinai Medical Center / Los Angeles, CA
Jennifer Kujak, MD Director of Oncological Imaging / RadNet Los Angeles / Los Angeles, CA
Clinical history:
- Age at diagnosis: 65
- Date of diagnosis: 12/2005
- PSA at diagnosis: Unknown
- Gleason score: 8
- Initial treatment: Radical prostatectomy (2/2006)
- Final pathology: pT2C, N0, M0
- Post treatment nadir PSA: 0.10 ng/mL (10/2006); remained undetectable through 8/2010
PSA at consultation:
- 4.5 ng/mL (11/2016)
Conventional imaging results:
- Negative Tc-99m bone scan (1/2017)
Planned clinical management:
- Salvage radiation to the prostatectomy bed
Details associated with decision to refer patients for an Axumin scan:
- Rising PSA 10+ years post-prostatectomy
- PSA at time of Axumin scan: 4.6 ng/mL (3/2017)
Axumin imaging interpretation:
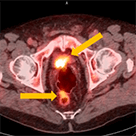
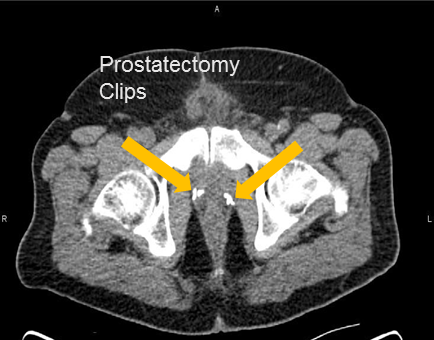
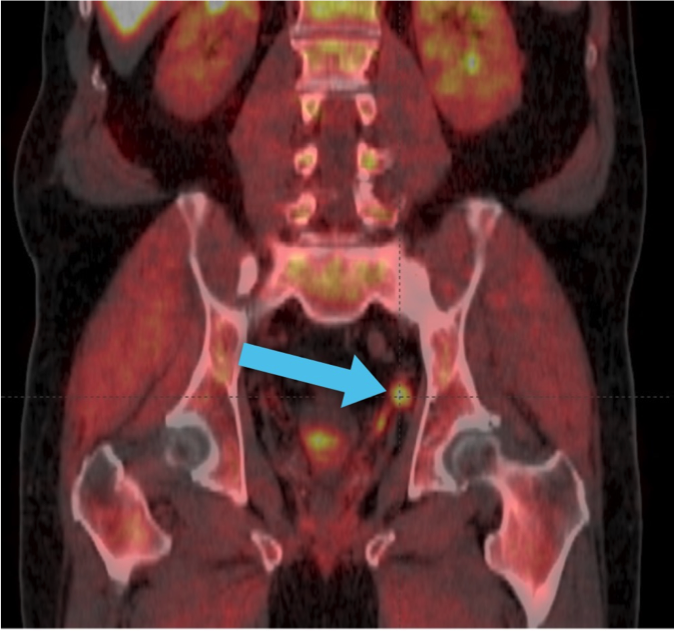
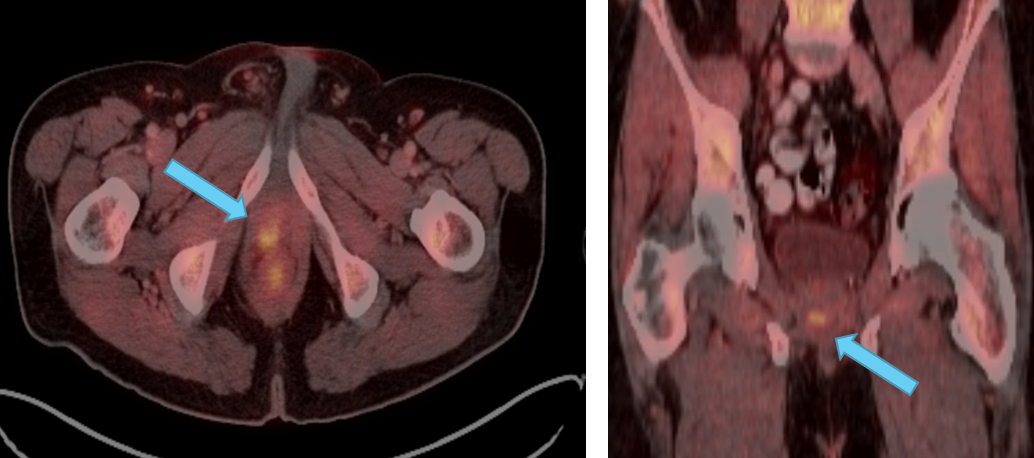
- Positive Axumin PET/CT: Fluciclovine F 18 uptake demonstrated in the left seminal vesicle and 8mm lymph node along the superior left pelvic side wall, adjacent to a surgical clip
Final management plan:
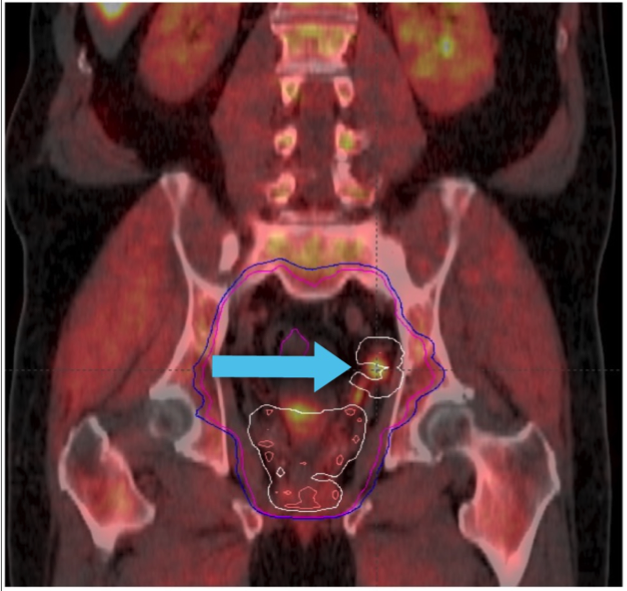
- With delineation of disease outside of the intended radiotherapy field, the management plan was revised to include pelvic radiotherapy with boost to Axumin avid disease, and androgen deprivation
Clinical follow-up:
- PSA on available short-term follow-up dropped significantly to 0.1 ng/mL (9/2017)
Axumin imaging revealed avid disease within the left seminal vesicle (3/2017)
Axumin imaging revealed avid 8mm lymph node along the superior left pelvic side wall, adjacent to a surgical clip (3/2017)
Provided by:
Barry A. Siegel, MD Professor, Sr. Vice Chair, and Chief / Division of Nuclear Medicine / Department of Radiology / Washington University / St. Louis, MO
Jeff M. Michalski, MD Vice Chairman, Radiation Oncology / Chief, Genitourinary Service / Washington University / St. Louis, MO

Clinical history:
- Age at diagnosis: 63
- Date of diagnosis: 11/2015
- PSA at diagnosis: 10.3 ng/mL
- Gleason score: 4+4=8
- Initial treatment: Radical prostatectomy (3/2016)
- Final pathology: pT3b, N1, M0
- Post treatment nadir PSA: 6.0 ng/mL (5/2016)
- Adjuvant treatment: leuprolide (6/2016)
- PSA 1.1 ng/mL (9/2016)
Conventional imaging results:
- Negative bone scan (9/2016)
- Negative CT scan (9/2016)
Additional PSA draws:
- 0.9 ng/mL (10/2016)
- 1.0 ng/mL (11/2016)
Planned clinical management:
- Salvage radiotherapy to the prostate bed and whole pelvis
Details associated with decision to refer patient for an Axumin scan:
- To investigate if nodal disease remained since PSA never became undetectable
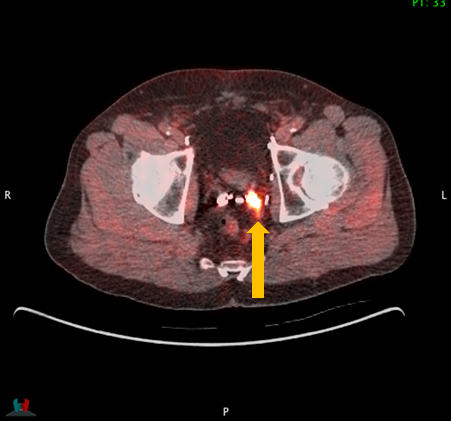
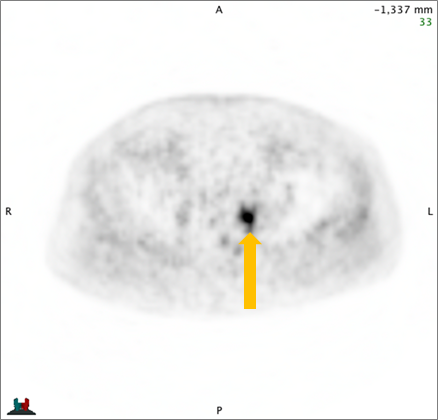
Axumin imaging interpretation:
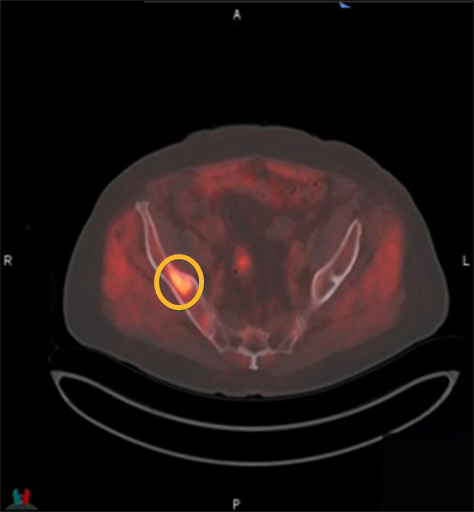
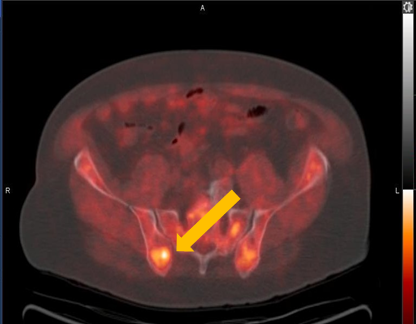
- Positive Axumin PET/CT: Fluciclovine F 18 uptake in left obturator lymph node (11/2016)
Final management plan:
- Salvage radiotherapy to the prostate bed and whole pelvis with boost to areas guided by Axumin imaging (3/2017); initiated ADT (leuprolide) for 24 months
Clinical follow-up:
- PSA: <0.1 ng/mL (12/2017)
Axumin imaging revealed left obturator lymph node positive uptake (11/2016)
Lymph Node SUV (bw)max: 3.2
Provided by:
Michael Kipper, MD Nuclear Medicine Physician / Genesis Research LLC / San Diego, CA
Paul Dato, MD Urologist / Genesis Research LLC / San Diego, CA
Clinical history:
- Age at diagnosis: 71
- Date of diagnosis: 11/2008
- PSA at diagnosis: 3.87 ng/mL
- Gleason score: 4+3=7
- Initial treatment: Radical prostatectomy (12/2008)
- Final pathology: pT2c, N0, M0; no extra prostatic and perineural extension; negative margins and seminal vesicles
- Post treatment nadir PSA: <0.10 ng/mL (12/2011)
PSA at recurrence:
- 2.66 ng/mL (1/2016)
- 3.40 ng/mL (6/2016)
Conventional imaging results:
- Negative CT scan (5/2016)
- Negative Tc-99m bone scan (6/2016)
Planned clinical management:
- Salvage radiotherapy to the prostate bed
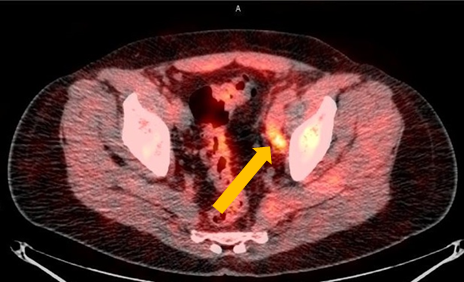
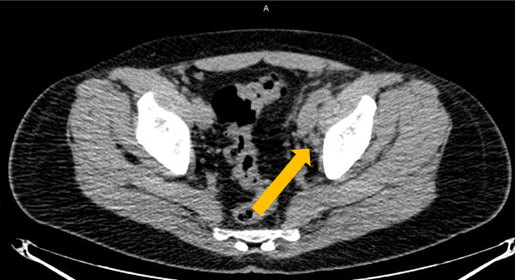
Axumin imaging interpretation:
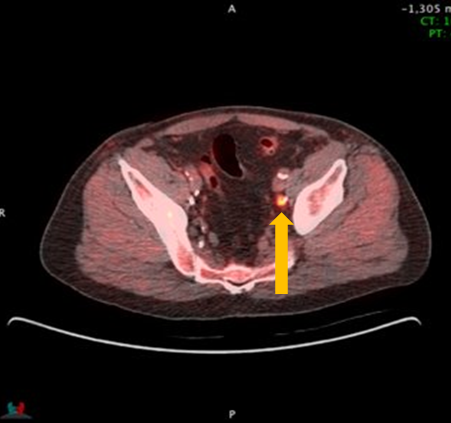
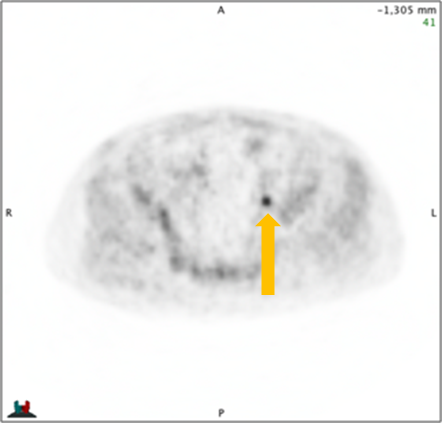
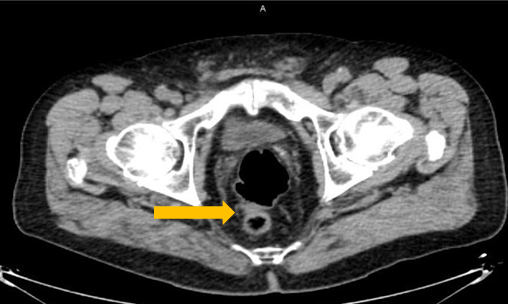
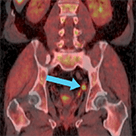
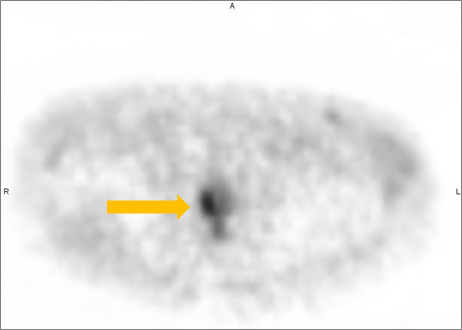
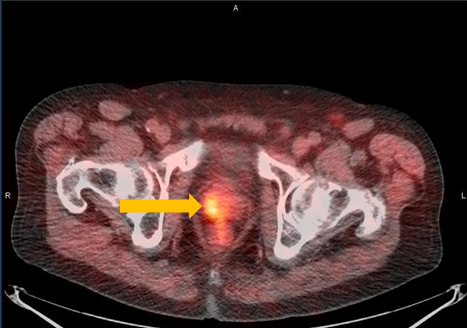
- Positive Axumin PET/CT: Fluciclovine F 18 uptake in anterior peri-rectal lymph node (6/2016)
Final management plan:
- Salvage radiotherapy to the prostate bed with boost to areas guided by Axumin uptake
Clinical follow-up:
- Leuprolide (7/2016)
- PSA: 0.30 ng/mL (8/2016)
- EBRT/IMRT (8/2016)
- PSA: <0.10 ng/mL (10/2016)
- PSA: <0.10 ng/mL (12/2016)
- Undetectable at follow up
Axumin imaging revealed interior peri-rectal malignant lymph node uptake (6/2016)
Lymph Node SUV(bw)max: 2.8
Blood pool SUV(bw)mean: 2.2
Provided by:
David Josephson, MD, FACS Tower Urology Institute for Minimally Invasive and Robotic Surgery / Attending Surgeon / Cedars Sinai Medical Center / Los Angeles, CA
Jennifer Kujak, MD Director of Oncological Imaging / RadNet Los Angeles / Los Angeles, CA
Bony Uptake
Clinical history:
- Age at diagnosis: 74
- Date of diagnosis: 3/2017
- PSA at diagnosis: 6.0 ng/mL
- Gleason score: 4+4=8
- Initial treatment: Robot assisted radical prostatectomy (6/2017)
- Final pathology: 4+3=7 with tertiary pattern 5 + perineurial invasion; seminal vesicle invasion and extra-prostatic extension, tumor present in both lobes, pT3c, Nx, Mx
- Post treatment nadir PSA: 0.11 ng/mL (9/2017)
PSA at recurrence:
- 1.29 ng/mL (1/2018)
- 1.88 ng/mL (2/2018)
Conventional imaging results:
- MRI (2/2018):
- Small pelvic lymphocoele
- Diffuse urinary bladder wall thickening may be sequela of prior chronic outlet obstruction
- No lymphadenopathy
- Small bilateral hydroceles
- No MR evidence of recurrent prostate cancer in the surgical bed and visualized pelvis
Planned clinical management:
- Radiotherapy to pelvic nodes with boost to prostatic fossa and short-course ADT
Details associated with decision to refer patient for an Axumin scan:
- Localize site of recurrence (3/2018)
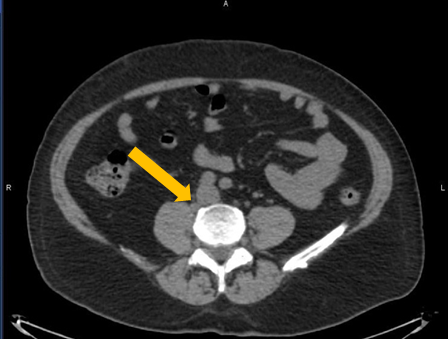
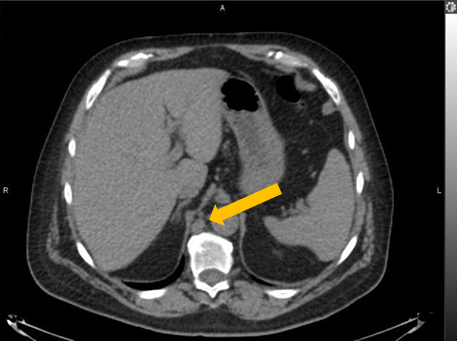
Axumin imaging interpretation:
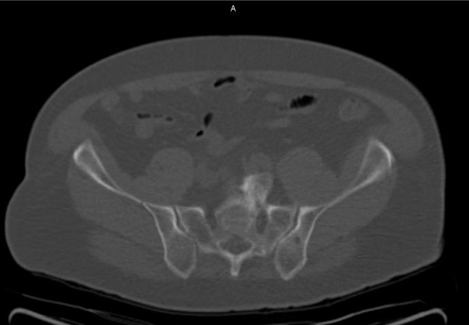
- Positive Axumin PET/CT: demonstrated asymmetric intense fluciclovine F 18 uptake localized to a sclerotic lesion in the middle right iliac bone
- Findings consistent with an isolated osseous metastasis
Final management plan:
- Stereotactic body radiation therapy to isolated iliac metastases plus short-course ADT
- PSA to be closely monitored
Provided by:
Froylan Gonzalez, MD Board Certified Urologist / Georgia Urology / Canton, GA
Clinical history:
- Age at diagnosis: 72
- Date of diagnosis: 1/2013
- PSA at diagnosis: 4.0 ng/mL
- Gleason score: 7
- Initial treatment: Radical prostatectomy (3/2013)
- Final pathology: pT2c, N0, MX
- Post treatment nadir PSA: 0.2 ng/mL (5/2013)
PSA at recurrence:
- 0.2 ng/mL (6/2015)
- 0.4 ng/mL (8/2016)
Conventional imaging results:
- Negative bone scan (8/2016)
- Equivocal MRI of prostate and prostate bed (8/2016)
Planned clinical management:
- ADT and salvage radiotherapy to the prostate bed
Axumin imaging interpretation:
- Positive Axumin PET/CT: Axumin scan demonstrated fluciclovine F 18 activity in right illium and left prostatectomy bed (8/2016)
Final management plan:
- ADT and salvage radiotherapy to the prostate bed and whole pelvis with boost to areas guided by Axumin uptake; leuprolide (8/2016); EBRT/IMRT (10/2016); EBRT/IMRT (11/2016)
Clinical follow-up:
- PSA response: <0.1 ng/mL (1/2017)
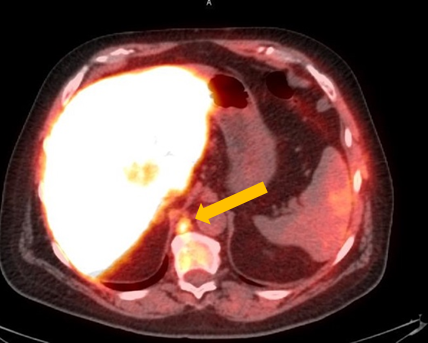
Axumin imaging revealed right Ilium skeletal uptake (8/2016)
Rt. Ilium Lesion SUV(bw)max: 6.0
Marrow (L3) SUV(bw)mean: 3.0
Axumin imaging revealed left prostatectomy bed uptake (8/2016)
Prostatectomy Bed Lesion SUV(bw)max: 4.3
Marrow (L3) SUV(bw)mean: 3.1
Provided by:
Barry A. Siegel, MD Professor, Sr. Vice Chair, and Chief / Division of Nuclear Medicine, Department of Radiology / Washington University / St. Louis, MO
Jeff M. Michalski, MD Vice Chairman, Radiation Oncology / Chief, Genitourinary Service / Washington University / St. Louis, MO
Clinical history:
- Age at diagnosis: 67
- Date of diagnosis: 2018
- PSA at diagnosis: 4.4 ng/mL
- Gleason score: 4+5
- Initial treatment: Robotic assisted laparoscopic radical prostatectomy and bilateral pelvic lymphadenectomy
- Final pathology: pT3pN0M0, stage IIB; Adverse features, including positive right bladder neck margin, focal extraprostatic extension, and diffuse perineural angiolymphatic invasion
- Post treatment nadir PSA: 0.15 ng/mL
PSA at recurrence:
- 0.9 ng/mL (8/2018)
Conventional imaging results:
- NaF bone scan: negative (2018)
Planned clinical management:
- Post-prostatectomy external radiation treatment (XRT)
Details associated with decision to refer patients for an Axumin scan:
- Scan will inform XRT volume planning
Axumin imaging interpretation:
- Positive Axumin PET/CT: Increased tracer uptake in the left pelvis
- No evidence of distant disease
Final management plan:
- XRT planning adjusted to incorporate Axumin PET/CT findings

Negative NaF PET/CT Bone Scan
Positive Axumin PET/CT scan
IMRT and daily IGRT to 45.0 Gy/1.8 Gy/25 treatments followed by an additional 23.4 Gy/1.8 Gy/13 treatments to the prostate bed to achieve a total treatment dose of 68.4 Gy/1.8 Gy/38 treatments
Provided by:
Steven Eric Finkelstein, MD, DABR, FACRO Florida Cancer Affiliates / The US Oncology Network
Prostate Bed Uptake
Clinical history:
- Age at diagnosis: 71
- Date of diagnosis: 3/2007
- PSA at diagnosis: 5.9 ng/mL
- Gleason score: 4+3=7
- Initial treatment: Radiotherapy - EBRT/IMRT (5/2007)
- Clinical stage: cT2a, M0, N0
- Post treatment nadir PSA: 0.7 ng/mL, remained stable until 1/2014
Additional treatment and PSA draws:
- PSA: 1.1 ng/mL (1/2014)
- Received short term leuprolide (8/2014) + docetaxel (9/2014)
- Progressive PSA rise to 10.8 ng/mL (1/2016)
- PSA: 8.6 ng/mL (2/2016)
- PSA: 7.8 ng/mL (6/2016)
Conventional imaging results:
- Negative CT scan (6/2016)
- Retroperitoneal lymph nodes, other lymph nodes, prostate and prostate bed
Planned clinical management:
- Androgen deprivation therapy (ADT)
Details associated with decision to refer patient for an Axumin scan:
- Rising PSA post-radiotherapy
Axumin imaging interpretation:
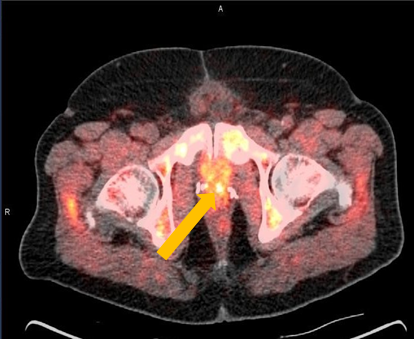
- Positive Axumin PET/CT: Abnormal fluciclovine F 18 activity demonstrated in the right mid-peripheral zone of the prostate with SUVmax of 3.4 (biopsy confirmed on 8/2016)
Final management plan:
- Salvage SBRT (9/2016)
Clinical follow-up:
- PSA: 1.1 ng/mL (1/2017)
- PSA: 0.3 ng/mL (3/2019)
- Continued observation
Axumin imaging revealed right mid peripheral zone malignant uptake (7/2016)
Prostate Lesion SUV(bw)max: 3.4
Marrow (L3) Reference SUV(bw)mean: 2.6
Provided by:
Michael Kipper, MD Nuclear Medicine Physician / Genesis Research LLC / San Diego, CA
Paul Dato, MD Urologist / Genesis Research LLC / San Diego, CA
Clinical history:
- Age at diagnosis: 60
- Date of diagnosis: 11/2014
- PSA at diagnosis: 3.0 ng/mL
- Gleason score: 4+3
- Initial treatment: Whole gland HIFU (1/2015)
- Post treatment nadir PSA: 0.3 ng/mL
PSA at recurrence:
- 1.3 ng/mL (2/2016)
Subsequent PSA levels:
- 1.90 ng/mL (5/2016)
- 2.40 ng/mL (7/2016)
- 2.70 ng/mL (9/2016)
- 4.95 ng/mL (1/2017)
- 7.10 ng/mL (5/2017)
Conventional imaging results:
- MRI Prostate Protocol: Significantly limited exam secondary to severe prostatic atrophy and loss of zonal anatomy related to reported prior HIFU without definitive MRI findings to suggest prostate adenocarcinoma.
- Bone Scan: Negative
Planned clinical management:
- Considered for salvage prostatectomy, brachytherapy pending imaging studies.
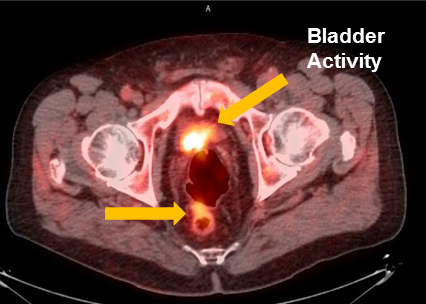
Axumin imaging interpretation:
- Positive Axumin scan with focal uptake is considered nonspecific but concerning for disease versus hypertrophy in the appropriate clinical setting.
Final management plan:
- After biopsy confirmation, patient was taken to the OR on 12/2017 for salvage whole gland brachytherapy.
Clinical follow-up:
- PSA
- Pre-Salvage: 7.1 ng/mL
- Post-Salvage (1.5 years): 0.03 ng/mL
- No evidence of disease approximately 1.5 years after salvage.
Provided by:
Jonathan Tward, MD, PhD Rudolph P. and Edna S. Reese Endowed Research Professor / Associate Professor of Radiation Oncology / Co-Leader, Genitourinary Malignancies Disease-Oriented Team / Huntsman Cancer Institute at the University of Utah
Clinical history:
- Age at diagnosis: 62
- Date of diagnosis: 2014
- Gleason score: 4+3=7
- Initial treatment: Radical prostatectomy (2014)
- Final pathology:
- No extracapsular extension, 2 nodes (benign), perineural involvement in the prostate, involvement of periprostatic adipose tissue, Gleason 7.
- Showed no tumor identified in seminal vesicles bases
- Post treatment nadir PSA: Undetectable
PSA at recurrence:
- Undetectable for 3 years
- 0.4 ng/mL (2018)
- 0.8 ng/mL (4/2019)
Conventional imaging results:
- CT scan: No adenopathy or bone lesions; stable pancreatic cystic mass (incidental) (5/2019)
- Bone scan: No concerning foci (5/2019)
Planned clinical management:
- Radiotherapy and androgen suppression
Details associated with decision to refer patients for an Axumin scan:
- Imaging needed to localize any sites of metastases
Axumin imaging interpretation:
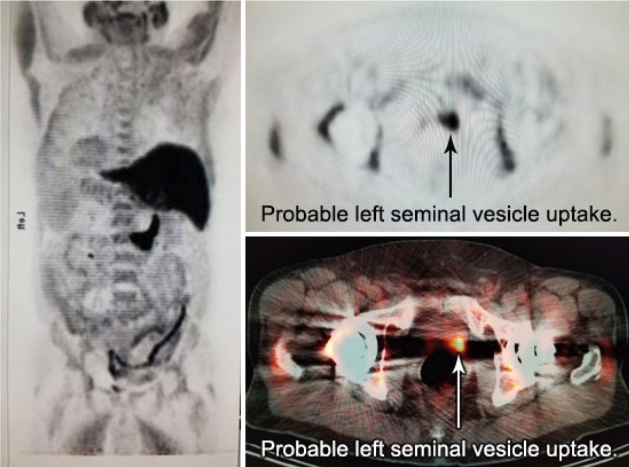
- Focus in the left seminal vesicle region amidst streak artifact reaches max SUV 6.4, favoring local malignant recurrence
Axumin impact on treatment plan:
- Axumin pinpointed the target for radiation not visible by other modalities
Final management plan:
- Underwent salvage radiotherapy (completed 8/2019) and androgen suppression
Follow-up and outcomes:
- Post-treatment PSA was 0.2 ng/mL as of September 2019
Provided by:
Shawn S. Carter, MD Radiology Regional Center / Fort Myers, Florida
These case studies are being provided to you as examples of the images and information available following Axumin PET/CT imaging in men with suspected prostate cancer recurrence based on elevated blood prostate specific antigen (PSA) levels following prior treatment. The responsibility for the accurate and timely acquisition and interpretation of images using Axumin PET/CT scanning rests with the nuclear medicine physician or radiologist supervising the PET/CT imaging facility. Axumin is not indicated for directing or changing patient management. These case studies are not intended to substitute for the independent medical judgment of the physician(s) responsible for the individual patient’s management, nor are they a guarantee of any specific clinical results. Incidental findings are noted in some of the cases, as examples of potential, unanticipated abnormalities that may be identified during interpretation of Axumin images. The diagnostic efficacy of Axumin for the identification of these incidental abnormalities has not been established and confirmatory testing may be considered appropriate. These case studies are post marketing, on label, and, at present, there is nothing to suggest that adverse events potentially change Axumin’s safety profile.
Reference:
- Andriole GL, Kostakoglu L, Chau A, et al. The impact of positron emission tomography with 18F-fluciclovine on the management of patients with biochemical recurrence of prostate cancer: results from the LOCATE trial. J Urol. 2019;201(2):322-331.
INDICATION
Axumin® (fluciclovine F 18) injection is indicated for positron emission tomography (PET) imaging in men with suspected prostate cancer recurrence based on elevated blood prostate specific antigen (PSA) levels following prior treatment.
IMPORTANT SAFETY INFORMATION
- Image interpretation errors can occur with Axumin PET imaging. A negative image does not rule out recurrent prostate cancer and a positive image does not confirm its presence. The performance of Axumin seems to be affected by PSA levels. Axumin uptake may occur with other cancers and benign prostatic hypertrophy in primary prostate cancer. Clinical correlation, which may include histopathological evaluation, is recommended.
- Hypersensitivity reactions, including anaphylaxis, may occur in patients who receive Axumin. Emergency resuscitation equipment and personnel should be immediately available.
- Axumin use contributes to a patient’s overall long-term cumulative radiation exposure, which is associated with an increased risk of cancer. Safe handling practices should be used to minimize radiation exposure to the patient and health care providers.
- Adverse reactions were reported in ≤1% of subjects during clinical studies with Axumin. The most common adverse reactions were injection site pain, injection site erythema and dysgeusia.
To report suspected adverse reactions to Axumin, call 1-855-AXUMIN1 (1-855-298-6461) or contact FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Please see Axumin full Prescribing Information.